Knee Replacement During your consultation, you will be given all the information you need about the procedure of your particular joint surgery. However, there are some techniques that we use to make your recovery time as short as possible and the relief as immediate as we can.
Where possible, hip surgery will be completed using minimally invasive techniques. This means that a hip prosthesis will be inserted through an incision that is generally less than 10cm. This involves more splitting and less cutting of the muscles, meaning that there is less blood loss, faster recovery and a more cosmetic scar.You may need to undergo knee surgery for a number of reasons, and so the type of implant or replacement will reflect this.
This is a hinge joint. It is lined by articular cartilage and has two fibro-cartilage structures (menisci) which lead to enhanced stability, transfer of joint forces and nutrition of the joint. Stability is further achieved by the cruciate ligaments in the centre and collateral ligaments at the periphery of the joint, as well as surrounding muscles.
Knee replacement surgery is usually necessary when the knee joint is worn or damaged so that your mobility is reduced and you are in pain even while resting. The most common reason for knee replacement surgery is osteoarthritis. Knee pain can significantly affect your mobility and overall quality of life. Consult with the best knee surgeon and take the right treatment

Knee Replacement, conjointly called knee surgical operation, may be a operation to switch the weight-bearing surfaces of the articulatio genus to alleviate pain and incapacity. it’s most typically performed for degenerative arthritis, and conjointly for different knee diseases like arthritis and atrophic arthritis. In patients with severe deformity from advanced arthritis, trauma, or long-standing degenerative arthritis, the surgery could also be a lot of sophisticated and carry higher risk. pathology doesn’t usually cause knee pain, deformity, or inflammation and isn’t a reason to perform knee replacement.
Other major causes of weakening pain embody gristle tears, animal tissue defects, and ligament tears. weakening pain from degenerative arthritis is far a lot of common within the old.
Knee Replacement surgery is performed as a partial or a complete knee replacement. generally, the surgery consists of commutation the pathological or broken joint surfaces of the knee with metal and plastic elements formed to permit continued motion of the knee.
The operation usually involves substantial surgical pain, and includes vigorous rehabilitation. The recovery amount could also be twelve weeks or longer and will involve the employment of quality aids (e.g. walking frames, canes, crutches) to change the patient’s come back to surgical quality.[3] it’s calculable that roughly eighty two of total knee replacements can last twenty five years.
Total Knee Replacement
The traditional technique for repairing a broken knee could be a total knee replacement surgery (TKR).
Since the primary operation in 1968, doctors have dramatically improved the procedure. In fact, advancements in medical technology have crystal rectifier to specific and extremely purposeful artificial knee implants that just about duplicate the means the human knee moves — and ar custom suitable your body. A TKR is currently among the safest and best of all commonplace orthopaedic surgeries.
During a TKR, a medico removes the surface of your bones that are broken by degenerative arthritis or alternative causes and replaces the knee with a man-made implant that’s elite to suit your anatomy. The medico uses special surgical instruments to chop away the rheumatoid bone accurately so form the healthy bone beneath to suit exactly into the implant elements.
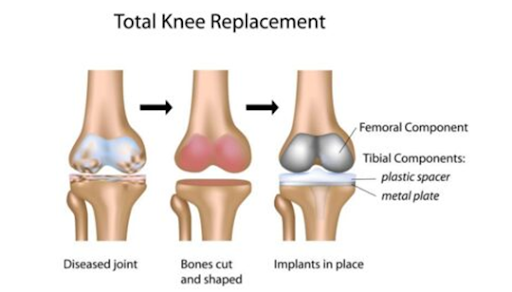
Essentially, the surgery could be a four-step method. the primary half involves getting ready the bone by removing the broken gristle surfaces at the ends of the femur (femur) and tibia (tibia), similarly as alittle portion of underlying bone.
During consequent part, the medico positions the metal leg bone and leg bone implants and either cements them to the bone or press-fits them. “Press-fitting” refers to implants that designed with rough surfaces to encourage the bone in your knee to grow into them, therefore securing the implants organically.
The next step is to insert a plastic button beneath the kneecap (patella). this might need resurfacing the face of the kneecap so as to higher affix it to the button.
Finally, the medico implants a medical grade plastic spacer between the leg bone and leg bone metal elements so as to make a swish surface that glides simply and mimics the motion of the natural knee. so as to confirm a flourishing outcome, the medico should align the implants exactly and punctiliously work them to the bone.
The yankee Academy of orthopedic Surgeons reports that ninety p.c of these who’ve undergone TKR expertise a dramatic reduction in knee pain and take pleasure in improved quality and movement. Most ar able to resume daily activities.
However, it’s vital to line correct expectations and avoid high-impact activities like running and athletics. Moderate use of your artificial knee can increase the percentages that the implant can last for several years. regarding eighty five to ninety p.c of TKR implants still work well fifteen to twenty years when the operation.
Be aware that there ar risks ar related to a TKR. These risks embody infection that would lead to extra surgery, blood clots that would result in stroke or death, and continued knee instability and pain. A TKR conjointly needs AN extended program and residential aiming to accommodate the recovery amount. you must arrange on employing a walker, crutches, or a cane straightaway when surgery.
In addition, implant loosening or failures will occur — particularly if placement occurred between the implant and also the bone throughout surgery or subsequently. though these failures ar uncommon, and typically occur within the weeks following the first surgery, they might need a come back to the surgery for a revision surgery. throughout this procedure, the medico removes the unsuccessful implant, yet again prepares the bone, and installs a brand new implant.
Partial Knee Replacement
Partial knee replacement (PKR), generally noted as a uni-compartmental knee replacement, is associate possibility for atiny low share of individuals. so much fewer PKRs square measure performed than TKRs within the u. s..
As the name implies, solely a district of the knee is replaced so as to preserve the maximum amount original healthy bone and soft tissue as attainable. Candidates for this kind of surgery usually have degenerative joint disease in just one compartment of their knee. therefore surgery takes place in any of 3 anatomical compartments of the knee wherever morbid bone presents the foremost pain: the medial compartment settled on the within of the knee, the lateral compartment on the skin of the knee, or the patella limb compartment that’s positioned on the front of the knee between the leg bone and kneecap.
During a PKR, a doc removes the unhealthy portion of the knee — together with bone and animal tissue — and replaces that compartment with metal and plastic elements.
A PKR surgery offers many key blessings, together with a shorter hospital keep, quicker recovery and rehabilitation amount, less pain following surgery, and fewer trauma and blood loss. Compared with people who receive a TKR, those that receive a PKR typically report that their knee bends higher and feels additional natural.
However, there’s less assurance that a PKR can scale back or eliminate the underlying pain. and since the preserved bone remains prone to inflammatory disease, there’s additionally a larger probability that follow-up TKR surgery is also needed at some purpose within the future.
Surgeons sometimes perform PKRs on younger patients (under age 65) UN agency have many healthy bone remaining. The procedure is performed on one in all the 3 knee compartments. If 2 or additional knee compartments square measure broken, it’s most likely not the most effective possibility.
PKRs square measure most fitted for people who lead a lively manner and would possibly need a follow-up procedure — maybe a TKR — in twenty years some, when the primary implant wears out. However, it’s additionally used for a few older people UN agency live comparatively inactive lifestyles.
Because a PKR is a smaller amount invasive and involves less tissue, you’re doubtless to be up and concerning sooner. In several cases, a PKR recipient is ready to maneuver around while not the help of crutches or a cane in concerning four to 6 weeks — some 0.5 the time for a TKR. They additionally expertise less pain and higher practicality — and report high levels of satisfaction.
Types of Knee Replacement Approaches
Your doctor will opt for a surgical approach (as well because the approach to anaesthesia, whether or not general or regional) that’s best suited to your wants. You and also the medical team can interact in pre-operative coming up with that covers the sort of procedure you receive and associated medical needs.
In order to confirm a swish procedure, a talented orthopaedic operating surgeon can map your knee anatomy ahead so they’ll set up their surgical approach and anticipate special instruments or devices. this is often a necessary a part of the method. doable procedures area unit mentioned below.
Traditional surgery
In the ancient approach, the operating surgeon makes associate degree 8- to 12-inch incision and operates on the knee mistreatment customary surgical technique. Generally, the incision is formed on the front and toward the center (midline or anteromedial) or on the front and to the aspect (anterolateral) of the knee.
The traditional surgical approach sometimes involves cutting into the quadriceps femoris sinew so as to show the kneecap over and expose the rheumatic joint. This approach generally needs 3 to 5 recovery days within the hospital and regarding twelve weeks of recovery time.
Minimally invasive surgery
A operating surgeon could counsel a minimally invasive surgery (MIS) that reduces trauma to tissue, lessens pain, and reduces blood loss — consequently rushing recovery. A minimally invasive approach reduces the incision to three to four inches. A key distinction between this approach and also the customary surgery is that the kneecap is pushed to the aspect instead of being turned over. This ends up in a smaller turn over the {quadriceps|quadriceps femoris|musculus quadriceps femoris femoris|quad|extensor muscle|extensor} sinew and fewer trauma to the quadriceps muscle. as a result of the operating surgeon cuts less muscle, healing happens quicker, and you’re probably to expertise higher vary of motion once recovery.
The procedure modifies the techniques utilized in ancient surgery whereas mistreatment constant implants from ancient surgery. makers offer specialised instruments that facilitate to put the implant accurately however conjointly afford incisions to be created as tiny as doable. Since the sole amendment between MIS and ancient surgery is within the surgical technique, the semipermanent clinical outcomes area unit similar.
Types of minimally invasive approaches include:
Quadriceps-sparing approaches
After creating a token incision, the operating surgeon shifts the kneecap to the aspect and cuts away the rheumatic bone while not cutting through the quadriceps femoris sinew. The quadriceps-sparing technique, because the name suggests, is a smaller amount invasive than ancient surgery. It spares the quadriceps femoris muscle from the maximum amount trauma as doable.
Another term for this approach is “subvastus” as a result of access to the joint is taken from underneath (sub) the vastus muscle (the largest a part of the quadriceps femoris muscle group).
Another variation of a quadriceps-sparing approach is named midvastus. It conjointly avoids cutting the quadriceps femoris sinew, however rather than fully economical the vastus muscle by sinking it, during this surgical approach the muscle is split on a natural line through the center. the choice to use one approach versus another depends on the condition of your knee and close tissues.
The subvastus and midvastus approaches typically take longer to perform however could lead to a quicker rehab method. this is often as a result of there’s very little to no trauma to the underlying thigh muscle, creating it easier to run sooner once the operation.
Lateral approach
This approach is never used. It’s a lot of common for those whose knees tend to bend outward. The operating surgeon enters the ginglymus laterally, or from the aspect of the knee. The lateral approach is a smaller amount invasive than ancient surgery as a result of it spares abundant of the quadriceps femoris, creating it easier for patients to come to walking quicker.
Minimally invasive surgery trims the hospital keep to 3 to four days and it will shorten the recovery amount to four to 6 weeks. folks that get a PKR toughened less pain and were ready to resume daily activities quicker and higher than those that had customary surgery. At one year, however, there have been no vital variations between the 2 teams.
Minimally invasive approaches aren’t acceptable for everyone. Surgeons fastidiously value every patient and choose the approach that’s best. Also, minimally invasive surgery is tougher to perform and needs a a lot of specific technique, instruments, and surgical coaching. One study found that it needs regarding one hour longer than a conventional surgery. Consult your operating surgeon to debate your choices.
Computer-assisted surgery (CAS)
Increasingly, surgeons are turning to computer-assisted strategies for each TKRs and PKRs involving each ancient and minimally invasive procedures. A operating surgeon enters a patient’s anatomical information into a pc — a method known as “registration” — and also the pc generates a 3D model of the knee.
The package provides the operating surgeon with a a lot of precise, computer-aidedimage of the knee. the pc helps the operating surgeon align the knee elements a lot of exactly within the bone and will increase the percentages that the device can work effectively.
A computer-based approach conjointly permits a operating surgeon to control with a smaller incision and edges the patient by reducing recovery time. A a lot of precise match may scale back wear and increase the longevity of the new joint.
Frequently asked questions
Age, activity level, surgical history and a person’s weight can contribute to implant failure. Younger, active patients, people who are obese, and those who have had prior knee surgeries all have a higher increased risk of a failed implant.
Younger, more active patients have a higher rate of revision than older, less active patients because they place more stress on their prosthesis over more time. Obese patients have a higher incidence of wear and loosening because of the increased force of their weight, and they are more prone to infections because of their increased risk of wound healing. Patients with previous knee surgeries are at higher risk for infection and implant failure.
The most common symptoms of a failed knee implant are pain, decrease in joint function, knee instability, and swelling or stiffness in the knee joint.
Persistent pain and swelling can indicate loosening, wear or infection, and the location of the pain can be all over the knee (generalized) or in one particular area (localized). A decline in knee function may result in a limp, stiffness or instability. Patients who demonstrate these symptoms and signs may require revision joint surgery.
Revision total knee replacement is the replacement of a failed total knee prosthesis with a new prosthesis. In simple terms, it is the replacement of a knee replacement (or a “second knee replacement”).
Knee revision surgery is a complex procedure that requires extensive preoperative planning, specialized implants and tools, prolonged operating times, and mastery of difficult surgical techniques to achieve a good result.
When the decision for revision knee replacement is made, the surgeon will do a thorough clinical exam and order X-rays and laboratory tests. If infection is suspected, aspiration of the knee (joint fluid removed with a needle) may be required. The aspirated fluid will then be sent to a laboratory for analysis to identify the specific type of infection.
In addition to X-rays, other imaging modalities may be helpful, such as bone scans, CT scans or Magnetic Resonance Imaging (MRI). These advanced imaging technologies can demonstrate changes in the position or condition of the prosthetic components as well help to pinpoint the cause, location and the amount of bone loss to help plan for the surgery.
First, the old implant is removed and, if needed, bone grafts are used to fill any voids where bone has deteriorated. Then the new prosthesis is placed.
Most revision total knee replacements take longer to perform than primary procedures (about two to three hours).
Postoperative care is very similar to that after a primary knee replacement. This includes physical therapy, blood management, pain medication as necessary, antibiotics and some method of blood clot prevention. A brace or splint may be used to protect the joint after the surgery.
It varies, but in most cases, physical therapy will be initiated within 24 hours of the procedure and will continue for up to three months.
Some patients take longer to recover. In some cases, protective weightbearing or limiting the knee’s range of motion is needed to promote appropriate healing. Therapy will usually continue for up to three months following the surgery. Assistive devices, such as a walker or crutches, will be used early in the convalescence period, and patients will progress to a cane or walking without any assistance as their condition improves.
Any surgery can have potential complications. The complexity of revision joint surgery increases the chance of surgical complications, which include but are not limited to:
- wound drainage
- infection
- bleeding
- damage to nerves or blood vessels
- intra-operative fractures
- blood clot (deep vein thrombosis, DVT)
- pulmonary embolism
Infection, bleeding, damage to nerves or blood vessels, and intra-operative fractures can be minimized by using antibiotics before and after surgery, employing sterile surgical techniques and utilizing well-planned surgical exposures. Patients who are obese are particularly at increased risk of infection and wound drainage issues post operatively.
Similar to primary knee replacement, some mild swelling of the knee or ankle may be present after surgery for as long as three to six months. Swelling can be treated by elevating the leg, applying an ice pack, and wearing compression stockings.
Prior medical conditions, such as heart and lung complications or stroke conditions, can be aggravated by a revision procedure. These conditions may also develop in patients after revision surgery. Very rarely, death can occur. The decision to perform revision joint surgery is made when the benefits of pain relief and functional improvement outweigh the risk of potential complications.
Most patients who undergo revision procedures can expect to have good to excellent results. Although expected outcomes include pain relief with increased stability and function, complete pain relief and restoration of function is not always possible.
Up to 20% of patients may still experience some pain following revision knee surgery. This can persist for several years after the procedure. Additionally recovery after revision total knee surgery is heavily dependent on the state and function of the knee prior to the revision surgery.